Emergency Medicine Simulation: Training Clinicians for High-Stakes Decisions
Emergency medicine is the specialty where clinical errors have the least tolerance. A missed diagnosis or delayed intervention in a trauma bay carries consequences that cannot be undone. Traditional medical education prepares students for ambulatory and elective clinical encounters far more effectively than it prepares them for the chaotic, time-compressed environment of an emergency department. Simulation training closes that gap by creating controlled but realistic emergency scenarios where learners can build the skills, habits, and decision frameworks they will need when every second matters.
Why Emergency Medicine Demands Simulation
The emergency department exposes clinicians to a breadth of pathology that no other setting matches. In a single shift, a physician may manage acute MI, pediatric respiratory distress, polytrauma, septic shock, and acute psychiatric crises. The cognitive demands of rapidly prioritizing, diagnosing, and treating these patients simultaneously require a level of pattern recognition and procedural fluency that can only be developed through extensive practice.
Medical school and early residency cannot guarantee that every trainee will encounter sufficient emergency cases to develop these skills. Simulation solves the exposure problem. A well-designed simulation curriculum can systematically expose trainees to rare but high-acuity scenarios — tension pneumothorax, anaphylaxis, malignant arrhythmias — ensuring that every graduate enters independent practice having managed these conditions in a safe, supervised environment.
Core Simulation Modalities in Emergency Training
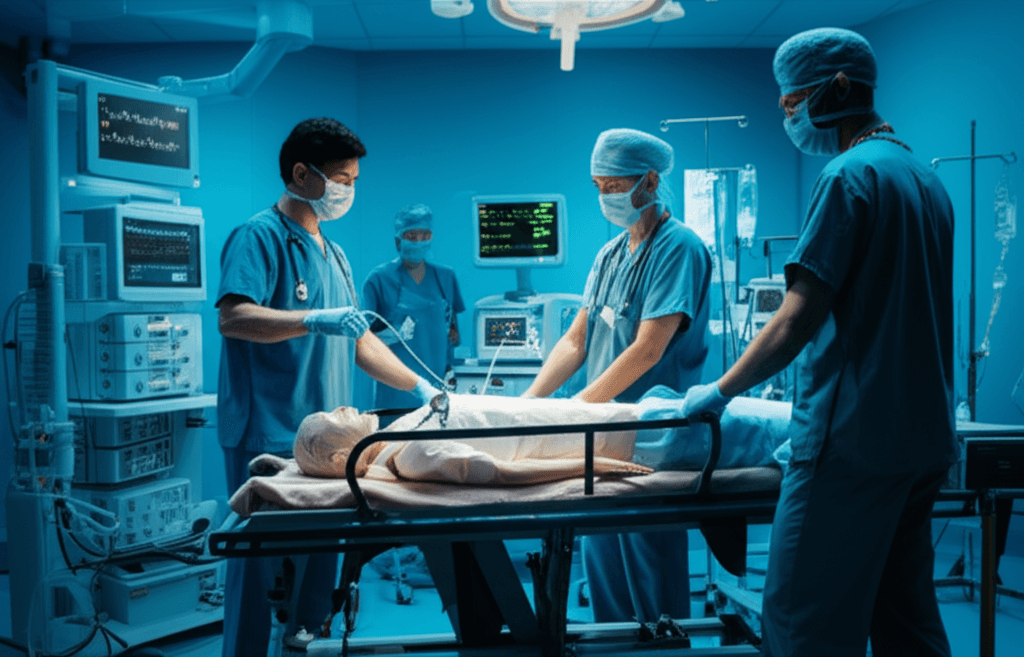
High-fidelity mannequins remain the gold standard for procedural emergency simulation. Intubation, central line placement, needle decompression, and pericardiocentesis all require tactile practice that screen-based systems cannot replicate. Emergency medicine programs typically maintain a mannequin-based simulation suite where trainees practice advanced procedures under supervision, make mistakes in safety, and receive immediate technical feedback.
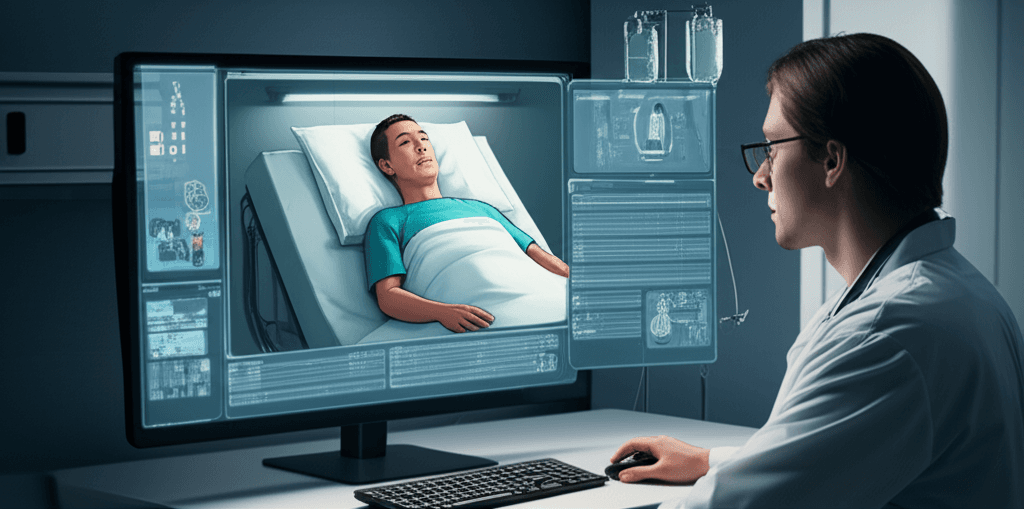
Virtual patient platforms complement procedural simulation by focusing on cognitive skills: history-taking under time pressure, differential diagnosis generation for undifferentiated presentations, and clinical decision-making with incomplete information. A virtual patient presenting with chest pain and nonspecific ECG changes forces the learner to work through a broad differential, order appropriate diagnostics, and initiate treatment based on evolving results — the same cognitive challenge they will face with a real patient, but without the risk.
Scenario Design for Emergency Simulation
Effective emergency simulation scenarios are built around learning objectives, not just clinical excitement. The goal is not to create the most dramatic scenario possible but to present situations that reliably expose specific cognitive or procedural gaps. A scenario designed to address anchoring bias, for example, might present a patient whose initial presentation strongly suggests one diagnosis but whose clinical course reveals a different underlying pathology. The learner's response to evolving information reveals whether they can update their mental model when new data contradicts initial impressions.
Scenarios should also address teamwork and communication, which are as critical in emergency care as technical skills. CRM concepts — closed-loop communication, situational awareness, task distribution — can be embedded into simulation scenarios and assessed during debriefing. Emergency medicine teams that train together in simulation demonstrate measurably better coordination in real resuscitations.
Integrating Emergency Simulation into Curricula
The most effective emergency simulation programs are longitudinal rather than event-based. Rather than isolated simulation days, trainees encounter simulation throughout their training at increasing levels of complexity. Early learners practice primary assessment and basic interventions. Advanced residents manage simultaneous patient presentations, team leadership, and resource allocation decisions. Each stage builds deliberately on the previous one.
Assessment in emergency simulation should move beyond subjective faculty impressions. Validated tools like the Ottawa Emergency Medicine Competency Assessment Tool (ECAT) provide structured frameworks for evaluating performance across domains. Video review of simulation sessions, with the learner present, is among the most effective feedback mechanisms available — it removes subjective disputes about what happened and focuses discussion on observable behavior and decision-making.