Case-Based Learning in Medical Education: Evidence and Implementation
Case-based learning has been a cornerstone of medical education since the Socratic method was first applied to clinical teaching. The fundamental principle is straightforward: students learn clinical reasoning most effectively when they work through realistic clinical scenarios that require them to integrate knowledge, analyze information, and make decisions. While the principle is old, the methods for implementing case-based learning continue to evolve as new technologies create possibilities that were not available a decade ago.
This article examines the evidence for case-based learning in medical education, distinguishes it from related pedagogical approaches, and provides practical guidance for curriculum designers who want to implement or strengthen case-based learning in their programs.
For curriculum committees considering educational innovation, case-based learning represents one of the most evidence-supported and practically achievable improvements available. Unlike some educational technologies that require significant infrastructure investment, case-based learning can be implemented with minimal additional resources when supported by the right digital tools and facilitation strategies.
Case-Based Learning vs Problem-Based Learning: Clarifying the Distinction
Case-based learning and problem-based learning are frequently confused or used interchangeably, but they are distinct pedagogical approaches with different structures and different faculty roles. Understanding the distinction matters because each approach serves different educational objectives and requires different implementation strategies.
Problem-based learning presents students with an ill-defined problem and asks them to identify learning objectives, research relevant knowledge independently, and reconvene to discuss their findings. The facilitator guides the process but does not teach content directly. Learning objectives emerge from the group discussion rather than being predefined by faculty.
Case-based learning presents students with a structured clinical case and guides them through a defined set of learning objectives. The facilitator actively directs the discussion, provides information at appropriate points, and ensures that key learning points are addressed. Cases are designed to cover specific content areas, and the session follows a planned trajectory.
For clinical reasoning development, case-based learning tends to be more efficient because the clinical content is controlled and comprehensive. For developing self-directed learning skills and collaborative problem-solving, problem-based learning offers distinct advantages. Many programs use both approaches at different points in the curriculum.
The Evidence Base for Case-Based Learning
Research on case-based learning in medical education consistently shows benefits in knowledge retention, clinical reasoning skills, and student engagement compared to lecture-based instruction alone. Multiple systematic reviews have found that students in case-based learning programs demonstrate better diagnostic accuracy, more systematic clinical reasoning approaches, and greater ability to transfer knowledge to novel clinical situations.
The mechanism behind these improvements is well understood from cognitive science. Case-based learning activates deeper cognitive processing than passive learning methods. When students must analyze clinical data, generate hypotheses, and justify decisions, they create richer memory structures that are more readily recalled in similar clinical situations. This is the same principle that explains why clinical experience is more valuable than textbook study: active engagement with clinical problems builds clinical expertise.
Student satisfaction with case-based learning is consistently high across studies. Students report that case-based sessions are more engaging than lectures, more relevant to their future clinical practice, and more effective at developing skills they believe they will need as physicians. This satisfaction is not trivial; engaged students learn more effectively than disengaged ones.
The evidence also suggests that case-based learning improves knowledge transfer to novel clinical situations. Students trained with cases develop mental frameworks for clinical reasoning that they can apply to unfamiliar presentations, not just the specific conditions covered in their training cases. This transfer effect is particularly valuable because clinical practice constantly presents physicians with patient presentations they have never encountered in exactly that form. The reasoning patterns developed through case-based practice provide the cognitive tools for approaching these novel situations systematically.
Designing Effective Clinical Cases
The quality of case-based learning depends entirely on the quality of the cases. A poorly designed case produces confusion rather than learning. An effective clinical case has several characteristics: clear learning objectives that align with curriculum goals, realistic clinical details that mirror authentic practice, an appropriate level of complexity for the target audience, and built-in decision points that require students to apply clinical reasoning rather than recall facts.
Cases should present information progressively, mimicking the way clinical data becomes available in real practice. The student receives an initial presentation, decides what history to take and what examinations to perform, receives results, and adjusts their clinical approach based on new information. This progressive disclosure structure is far more effective than presenting all case information simultaneously.
Include distractors and red herrings that require students to distinguish relevant from irrelevant information. In real clinical practice, not every symptom is significant and not every lab result is abnormal. Cases that present only relevant information train students to expect that everything they see matters, which is poor preparation for clinical reality.
Technology-Enhanced Case-Based Learning
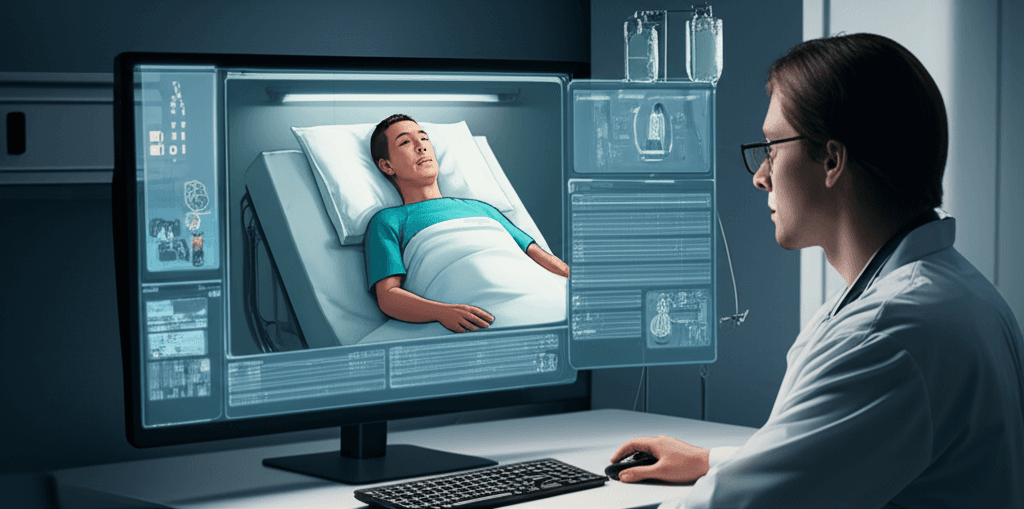
Virtual patient platforms have transformed what is possible in case-based learning. Traditional paper-based cases present text and ask students to discuss their responses in small groups. Virtual patient platforms create interactive clinical environments where students individually work through cases, making decisions that affect patient outcomes in real time.
The advantages of technology-enhanced case-based learning include scalability, individualization, and assessment granularity. Every student works through the complete case individually, making their own decisions rather than passively listening to peers in a group discussion. The platform tracks every decision, providing assessment data that would be impossible to collect in a group discussion format.
Virtual patient cases also provide immediate feedback that paper cases cannot. When a student orders an inappropriate test, the platform can show the result and let the student experience the consequences of their decision. When a student misses a critical finding, the patient's condition can deteriorate, demonstrating the clinical impact of the error. This consequential feedback drives learning more effectively than instructor correction after the fact.
Implementation Strategies for Curriculum Designers
Start by mapping your curriculum to identify where case-based learning will have the most impact. Clinical reasoning courses, integration weeks between basic science and clinical blocks, and pre-rotation preparation sessions are natural fit points. Do not attempt to replace the entire curriculum with case-based learning; target the areas where active clinical reasoning practice adds the most value.
Train facilitators specifically for case-based teaching. Facilitating a case discussion is a different skill than delivering a lecture. Facilitators need to manage group dynamics, ask probing questions, provide hints without giving away answers, and ensure that all learning objectives are addressed within the time constraint. Invest in facilitator development before launching case-based sessions.
Build assessment into every case from the design stage. Define what clinical competencies each case assesses, how performance will be measured, and what the passing criteria are. Cases that are educationally valuable but not assessed will be deprioritized by students who are rational about allocating their study time.
Measuring the Impact of Case-Based Learning
Assess impact at multiple levels. Immediate outcomes include student performance on case-specific assessments and student satisfaction ratings. Short-term outcomes include performance on clinical examinations that test the same competencies addressed by case-based sessions. Long-term outcomes include clinical rotation evaluations and ultimately clinical practice quality.
Compare student cohorts before and after case-based learning implementation, controlling for other curriculum changes. Track specific metrics: diagnostic accuracy scores, time to correct diagnosis, appropriateness of investigation ordering, and treatment plan quality. These granular metrics provide more actionable information than aggregate exam scores.
The strongest evidence for program effectiveness comes from longitudinal tracking. Students who receive extensive case-based learning should demonstrate measurably better clinical reasoning in their rotations and residencies compared to cohorts that received primarily lecture-based education. Establishing this longitudinal tracking requires institutional commitment to outcome measurement that extends beyond the immediate educational program.
Scaling Case-Based Learning Across the Curriculum
Successful case-based learning in one course often generates demand from other departments. Scaling from a single course to a curriculum-wide approach requires coordination, infrastructure, and institutional support that goes beyond individual faculty enthusiasm. Establish a curriculum committee subgroup specifically responsible for case-based learning integration to ensure consistency and prevent duplication across courses.
Create a shared case repository that faculty across departments can access, adapt, and contribute to. Cases developed for internal medicine can often be adapted for pharmacology, pathology, or public health courses with modification. A centralized repository prevents redundant case development effort and ensures that the institution's case library grows systematically rather than in isolated pockets.
Address the assessment alignment challenge early. As case-based learning expands across the curriculum, ensure that examination methods evolve to test the clinical reasoning skills that case-based sessions develop. An institution that teaches through cases but examines through multiple-choice recall questions sends contradictory signals to students about what matters. Align assessment with pedagogy, and case-based learning will fulfill its educational promise.