Obstetrics Simulation: Training for One of Medicine's Highest-Stakes Specialties
Obstetrics is a specialty where clinical excellence and catastrophic failure can be separated by a matter of minutes. Postpartum hemorrhage, shoulder dystocia, eclampsia, and neonatal resuscitation are emergencies that progress rapidly and demand coordinated responses from teams that may not have encountered these situations recently. Simulation training in obstetrics has accumulated strong evidence of effectiveness: institutions that implement regular obstetric simulation drills demonstrate measurable reductions in adverse maternal and neonatal outcomes.
Evidence for Obstetric Simulation Effectiveness
The evidence base for obstetric simulation is among the strongest in procedural simulation. A landmark study at a major academic medical center documented a 50% reduction in adverse maternal outcomes following the implementation of a structured obstetric emergency simulation program. Similar results have been replicated across diverse institutional settings, demonstrating that the benefits are not limited to academic centers with resources to build elaborate simulation programs.
The mechanisms underlying this improvement are well-understood. Obstetric emergencies require teams to execute specific protocols under time pressure with perfect communication. Simulation creates the practice opportunities that build procedural and communication fluency. Teams that have rehearsed their responses to shoulder dystocia or hemorrhage respond faster, communicate more clearly, and make fewer errors in real emergencies.
Core Obstetric Simulation Scenarios
Postpartum hemorrhage simulation must train teams in the systematic recognition of hemorrhage, the activation of massive transfusion protocols, the execution of uterotonic therapy, and the procedural interventions required when medical management fails. These scenarios are particularly effective when conducted in situ in the labor and delivery suite with real equipment, because they also assess system-level readiness — whether blood products are accessible, whether the suction equipment works, whether the team knows the protocol.
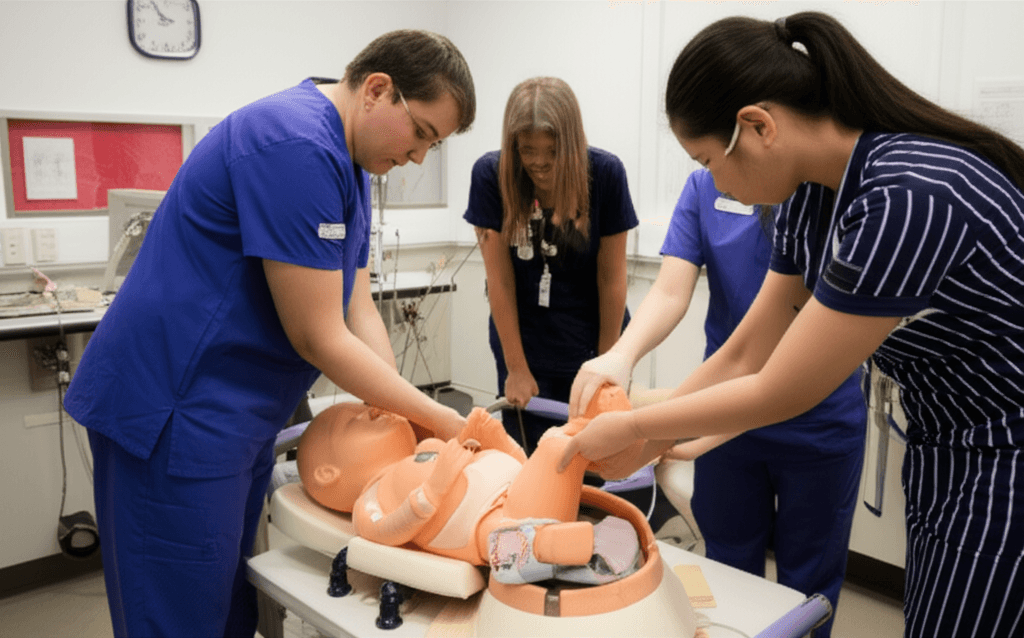
Shoulder dystocia simulation trains the specific sequential maneuvers — McRoberts, suprapubic pressure, internal rotational maneuvers, Gaskin all-fours — that must be executed in the correct order under time pressure. Mannequin-based simulation is uniquely suited to this training because it requires the physical application of technique in a realistic anatomical context. Teams that practice shoulder dystocia simulation demonstrate faster diagnosis-to-delivery intervals and more systematic maneuver execution in real events.
Neonatal Resuscitation Training
Every delivery carries the possibility of a neonate requiring resuscitation. The Neonatal Resuscitation Program (NRP) provides a structured protocol for managing the newly born infant who does not establish normal respiration and circulation. Simulation-based NRP training has become the global standard because it allows systematic practice of the assessment and intervention sequence in a format that can be updated as guidelines evolve.
Simulation of neonatal resuscitation is valuable not just for neonatologists and pediatricians but for all clinicians who attend deliveries. Family physicians, obstetricians, midwives, and labor and delivery nurses all need competency in initial newborn resuscitation because the neonatologist is not always present when a neonate needs immediate intervention.