Medical Simulation vs Traditional Lectures: Evidence-Based Comparison
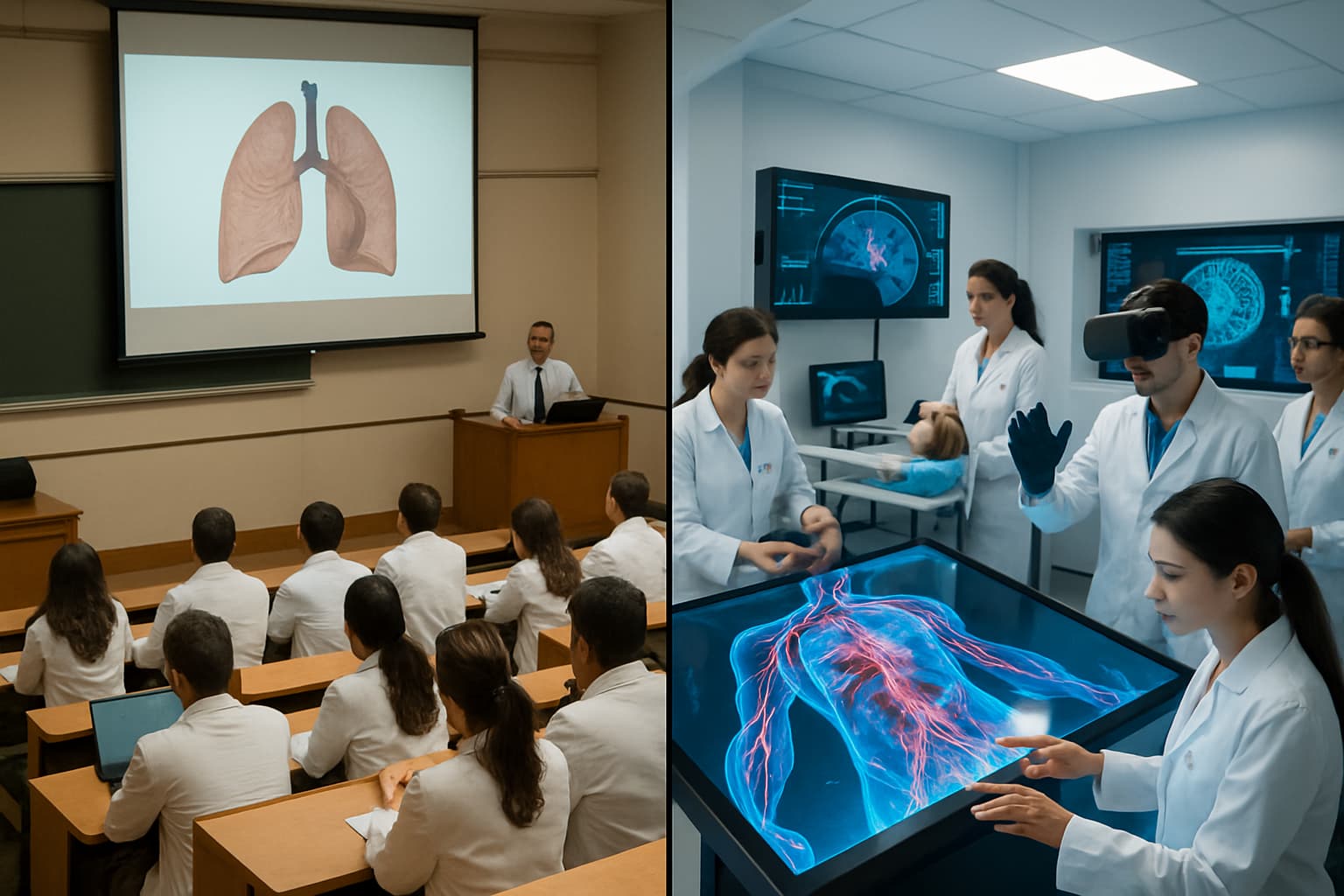
The debate between traditional lecture-based medical education and simulation-based learning is not theoretical. Decades of research in medical education have produced substantial evidence comparing the two approaches. The findings consistently favor active learning methods, including simulation, over passive lecture attendance for clinical skill development.
What the Research Shows
A landmark meta-analysis published in Academic Medicine examined over two hundred studies comparing simulation-based medical education to traditional methods. The findings were clear: simulation-based training produced consistently better outcomes in knowledge acquisition, clinical skills performance, and, in some studies, patient-level outcomes. The effect sizes were moderate to large, indicating educationally meaningful differences.
More recent research has focused on specific clinical domains. Studies in emergency medicine, surgery, and internal medicine have all demonstrated that students who receive simulation training perform better on objective clinical assessments than those who receive lecture-only instruction in the same topics.
Why Lectures Fall Short for Clinical Skills
Lectures are effective for transmitting factual information: the mechanism of action of beta-blockers, the stages of wound healing, the diagnostic criteria for diabetes. However, clinical practice requires more than factual recall. It requires the ability to apply knowledge in context, make decisions under uncertainty, and adapt approaches based on patient responses.
This application-level learning requires practice, and practice requires doing. A student can attend a lecture on cardiac auscultation and learn the acoustic characteristics of every murmur, but without actually listening to hearts, whether real or simulated, that knowledge remains theoretical. Simulation provides the doing that lectures cannot.
Knowledge Retention Differences
The retention curve for lecture-based learning is well documented and discouraging. Students typically retain less than half of lecture content after one week and substantially less after one month. Active learning methods, including simulation, show significantly better retention rates because they engage multiple cognitive pathways: visual, procedural, decision-making, and emotional.
When a student makes a diagnostic error in a simulation and sees the consequences, that experience creates a stronger memory trace than reading about the same error in a textbook. The emotional engagement of simulation-based learning, where students experience the stakes of their decisions even in a virtual environment, contributes to durable knowledge formation.
Student Engagement and Motivation
Medical students consistently report higher engagement and satisfaction with simulation-based learning compared to traditional lectures. This is not merely a preference; engagement correlates with learning outcomes. Students who are actively involved in their learning, making decisions, receiving feedback, and adjusting their approach, learn more effectively than those who passively receive information.
The interactive nature of simulation also addresses different learning styles. Visual learners benefit from 3D models and clinical scenarios. Kinesthetic learners benefit from procedural simulations. Analytical learners benefit from the diagnostic reasoning challenge. Lectures, by contrast, primarily serve auditory and reading-focused learners.
The Complementary Approach
The evidence does not suggest eliminating lectures entirely. Factual foundations are necessary, and well-designed lectures efficiently deliver baseline knowledge to large groups. The optimal approach combines structured content delivery with simulation-based practice: students learn the facts, then apply them in simulated clinical scenarios.
Medical schools that have adopted this blended model report that students enter clinical rotations better prepared, require less remediation, and demonstrate more consistent clinical performance. The cost of implementing simulation is offset by reduced remediation needs, improved student outcomes, and, ultimately, better-prepared physicians.